Genspect Australia has developed a deep knowledge of gender medicine in Australia through our clinician members, and through our support for parents, carers and others. We approach this subject without ideological or political baggage, motivated solely by a desire to see the best outcomes for children and young people and to support the parents and carers who also want the best for them.
The Genspect Australia team includes experienced professionals from diverse fields, including psychology, psychiatry, paediatrics, mental health nursing and general practice medicine. Some of our clinicians have previously worked in clinics that advocate for, or support hormonal interventions for gender dysphoria, and their experiences inform our concerns about current practices and models of care. Parents are also a key part of the team, bringing their experience of living in families impacted by gender distress.
Contents:
- How is gender dysphoria treated in Australia?
- What is gender identity?
- What about mental health?
- The correlation with neurodiversity and prior trauma
- Social influences on gender distress
- “Transing Away the Gay”
- The pathway from social transition and puberty blockers to cross-sex hormones
- Informed consent
- Emergence of regret and detransition
- More Information
How is gender dysphoria treated in Australia?
Australian state-run gender clinics primarily provide “gender affirming care” – a treatment model that recommends automatic acceptance of a young person’s stated gender identity without further exploration, followed by medical transition, if desired, to change their body in accordance with their internal sense of gender. For children this can include puberty blocking drugs that stop sex hormone release starting from age 9-10, and cross-sex hormone treatment from as young as age 14. This path may lead to later surgery, most commonly after age 18.
Most Australian children’s gender clinics reference the Australian Standards of Care and Treatment Guidelines for trans and gender diverse children and adolescents, developed by the Royal Children’s Hospital Melbourne. This document received a failing grade from an international review of guidelines, and has been the subject of much criticism – including in a decision of the Family Court. In early 2025, the National Health and Medical Research Council (NHMRC) announced it was reviewing the guidelines at the direction of the Australian Government.
Gender-affirming treatments for those over age 18 generally follow the Australian Informed Consent Standards of Care for Gender Affirming Hormone Treatment. This “informed consent” model places the responsibility for diagnosis and treatment decisions upon the patient, with the role of the clinician being to outline the risks and benefits and to support the patient’s decisions about gender transition that may include hormones and surgery. Mental health issues are not generally viewed as any significant obstacle to transition unless they affect the ability to consent. Guidelines from the controversial US-based World Professional Association for Transgender Health (WPATH) underpin Australian practice.
The NHMRC review, along with a decision by the Queensland Government and Northern Territory to pause puberty blocker and hormone prescription to minors, reflect growing international concerns about the safety and efficacy of these interventions. The National Health Service (NHS) England Cass Review, as well as systematic reviews from the UK, Europe, and Canada have found that the evidence for safety and efficacy of puberty blockers and cross-sex hormones for adolescents is of low or very low quality. Drawing on a large national cohort, a recent Finnish study of medical records found that severe psychiatric problems remained common and often worsened after medical gender reassignment in adolescents, indicating no clear mental‑health benefit from these interventions.
Genspect believes that the prescriptive, one-size-fits-all approach of the gender affirmation model risks misdiagnosing young people and encourages them down a path of medicalisation, with potentially lifelong and irreversible health consequences. Instead, Genspect advocates for an individualised approach. This means seeking to understand each young person’s unique circumstances, exploring the underlying factors that may have influenced their adoption of a transgender identity, and considering a tailored range of supports to meet their specific needs.
The long-term health consequences of puberty blockers and cross-sex hormones are little understood. Puberty blockers lead to reduced bone density, with additional concerns over possible effects on IQ and brain development. Together with cross-sex hormones they lead to sterility and likely loss of adult sexual function. Females taking testosterone suffer a number of known effects including incontinence, increased red blood cells and risk of stroke, increased risk of heart disease, vaginal and uterine atrophy with pelvic pain, and other suspected problems including liver damage and ovarian cancer risk. Males usually take a testosterone blocking drug as well as estrogen and this has known risks for thromboembolism (blood clots), meningioma (a normally benign brain tumour) and breast cancer. In light of the known risks and the absence of clear evidence of benefit, Genspect strongly urges against the use of these interventions.
What is gender identity?
Young people in Australia, along with their families and carers, are often told by gender clinics and school counsellors that gender identity is innate, that it is a deeply held sense of being male, female, or another gender, and cannot be influenced by social factors. However, this claim appears contradictory to another common assertion: that gender identity can be fluid. It is also not backed by the experience of detransitioners, or parents who have witnessed their children desist from their gender identity as they have matured.
Genspect believes that the problem with the concept of gender identity is that it relies on rigid gender stereotypes, when actually there is no one correct way for a man or woman, boy or girl, to behave, think or feel.
- Gender stereotypes are socially constructed ideas about how boys and girls should behave (e.g., “girls like pink, boys like trucks”; “girls are demure, boys are assertive”).
- Gender identity, as framed by gender clinics, is often described in ways that rely on gender stereotypes. For example, a child who prefers activities or clothing typically associated with the opposite sex may be encouraged to question their gender identity.
- Telling children they are “born in the wrong body” for liking certain toys or activities is regressive, and pathologises gender non-conforming behaviour. We believe children should be encouraged to freely and confidently express themselves, unrestricted by harmful gender stereotypes.
The reality is that very few people conform perfectly to traditional or stereotypical gender roles and preferences – everyone is an individual.
This conflation of gender identity with stereotypes may lead some young people to believe that discomfort with traditional gender roles means they must change their bodies to align with their gender identity. When this idea is reinforced by peers, social media, and even professionals, it can shape a young person’s understanding of themselves in ways that encourage them to pursue medical transition.
Genspect Australia is concerned that these social influences are driving the rapid rise in gender-related distress among young Australians, and further investigation is urgently needed.
What about mental health?
Many young people experiencing gender distress also have co-occurring mental health conditions (comorbidities). These can include:
- Depression
- Anxiety
- Post-traumatic stress disorder (PTSD), often linked to bullying or sexual assault.
Genspect recommends that young people and their families explore the conditions underlying gender dysphoria. Under the affirmation model, comorbidities are rarely considered significant or an impediment to medical intervention – particularly in clinics that follow the single-session assessment model. The affirmation model often prioritises pursuit of medical transition over other issues, thus delaying crucial evidence-based treatments.
Parents enrolling their children in gender clinics are often told that a multidisciplinary team will support their child’s psychological and social needs along with their medical needs. However, Genspect has observed that in practice, these services are primarily focused on affirming a child’s gender identity, while underlying mental health conditions may not be adequately addressed.
Parents are often placed under immense, and what we believe to be unconscionable, pressure to consent to puberty blockers or cross-sex hormones, often being told that their child is at high risk of self-harm or suicide without medical interventions. As parents, we understand how deeply distressing this messaging is, but we are also aware that peer-reviewed research shows that suicide in transgender-identified children and young people though somewhat elevated above their peers, is still rare, and there is no evidence that transition reduces suicidality. Self-harm and suicidal ideation are rarely the result of a single cause, and all distressed young people deserve a responsible, comprehensive response that ensures they receive appropriate psychological care, emotional support, and treatment for any underlying issues.
The correlation with neurodiversity and prior trauma
Genspect parents and clinicians have also observed a very high prevalence of neurodivergence, including autism and ADHD, among young people presenting with gender distress. International research confirms this overlap. Gender-affirmation advocates downplay or dismiss the association between autism and gender distress, and this is deeply concerning; even without a formal diagnosis, parents often recognise that their child’s neurodiverse traits make them particularly vulnerable to gender distress, warranting a cautious approach before irreversible medical decisions are made.
Many young people who do not yet fully understand the impact of autism spectrum traits, or of ADHD, often attribute the difficulties they experience to concerns about gender. There is similarly a high rate of traumatic experience in children with gender distress. Prior sexual assault may underlie a desire to change their body, especially for girls. Family breakdown is a common feature, and children in out-of-home care are over-represented.
Many detransitioners come to realise that transition was never a suitable treatment pathway to address difficulties associated with neurodiversity, trauma or mental health concerns.
Social influences on gender distress
The experience of Genspect clinicians and parents suggests that social factors are playing a significant role in promoting transgender identification and gender-related distress, including:
- Social media exposure
- Gender-focused groups and advocacy in schools
- Influence from peers and online communities
This is consistent with international research and the perspectives of former advocates of the affirmation model who have since reconsidered their stance.
Some argue that rising societal acceptance of diverse gender identities explains the rapid increase in transgender identification over the last decade. However, if this were the case, we would expect a more even distribution across age groups. Instead, the surge is overwhelmingly among adolescents and young adults, a period widely recognised as critical for identity formation. Evidence increasingly suggests that social factors, including a need for belonging, underpin this trend. Transgender communities offer young people, especially those who are neurodiverse and have long felt out of place, with a sense of acceptance and connection. However, in these groups they experience pressure to conform with a trans identity and to undertake medical transition.
“Transing Away the Gay”
Genspect is concerned that Australian gender clinics do not routinely seek to understand whether a young person identifying as transgender may, in fact, be same-sex attracted, and struggling with internalised homophobia. The Australian Standards of Care does not mention sexuality as a consideration. Some Australian clinics and proponents of the gender affirmation model have even reversed the well-established understanding of gender and sexuality – asserting that gender identity is innate and unchangeable, while suggesting that sexuality is fluid and influenced by external factors.
Yet, the relationship between gender identity and sexual orientation is complex and significant. Studies of detransitioners have found that a large proportion, in hindsight, believed their transition was partly driven by internalised homophobia. This is particularly evident among girls and young women, who as mature adults, come to understand their same-sex attraction. Other research indicates that, in the absence of social or medical transition, most pre-teen boys diagnosed with gender dysphoria grow up to be healthy gay or bisexual adults.
These findings warrant serious reflection. Are we truly supporting young people through the gender affirmation model, or are we, in some cases, reinforcing prejudices against same-sex attraction?
The pathway from social transition and puberty blockers to cross-sex hormones
Parents and young people are often told that puberty blockers are reversible, and are simply a “pause”—a way to give children time to explore their gender identity before making any permanent decisions. However, emerging evidence challenges these claims:
- Studies from gender clinics worldwide show that the vast majority—between 96% and 98%—of children who start puberty blockers proceed to cross-sex hormones. This strongly suggests that rather than providing time to think, puberty blockers reinforce a transgender identity and make medical transition more likely.
- When a child is socially affirmed as transgender—changing their name, pronouns, and sometimes dress and mannerisms—research suggests that it will psychologically reinforce the idea that transition is their only path forward. By the time they are old enough to consider medical options, their transgender identity has been solidified, making it harder to explore alternatives.
- Studies indicate that many children who experience gender distress ultimately desist and many grow up to be same-sex attracted adults. Blocking puberty may disrupt the natural process of physical, psychological and emotional maturation, instead pushing them toward permanent medical transition.
Informed consent
Genspect believes that everyone—especially parents and gender-distressed young people—needs clearer, more comprehensive information about the limitations of the evidence supporting medical intervention for gender dysphoria. Our experience suggests that gender clinics consistently present the science as settled, despite increasing medical debate and divided expert opinion.
We are particularly concerned that parents and young people are not properly informed about alternatives to the gender affirmation model such as psychotherapy. No one can provide truly informed consent without the knowledge of all available options.
Of great concern is the misinformation about the risk of self-harm and suicide, which can distort the consent process, particularly when families are already under enormous pressure. Some of our parents have experienced this firsthand. Presenting unevidenced claims of alarming rates of suicide is highly irresponsible and undermines ethical medical practice.
Emergence of regret and detransition
Parents and young people considering medical interventions for gender transition are often told that rates of regret and detransition are very low. But the reality is that we simply do not know the true rate of regret or detransition. A range of factors may contribute to the difficulty in assessing the full scope of detransition:
- Clinics rarely conduct systematic follow-up of patient outcomes
- Published studies have high patient drop out rates
- Follow-up periods may be short, and studies suggest regret takes an average of 7-10 years to develop
- Narrow definitions of regret, e.g. patients need to request surgery reversal
There have also been instances where researchers have withheld unfavourable follow-up data, further obscuring the true picture. The Australian Trans20 Study has been following 618 patients over time since 2017, but has not yet published any key findings.
Patients with regret over hormones and surgeries are emerging in Australia —and Genspect believes that understanding this phenomenon is essential to ensuring truly informed consent for those considering medical transition. For more information, see our detransition support page.
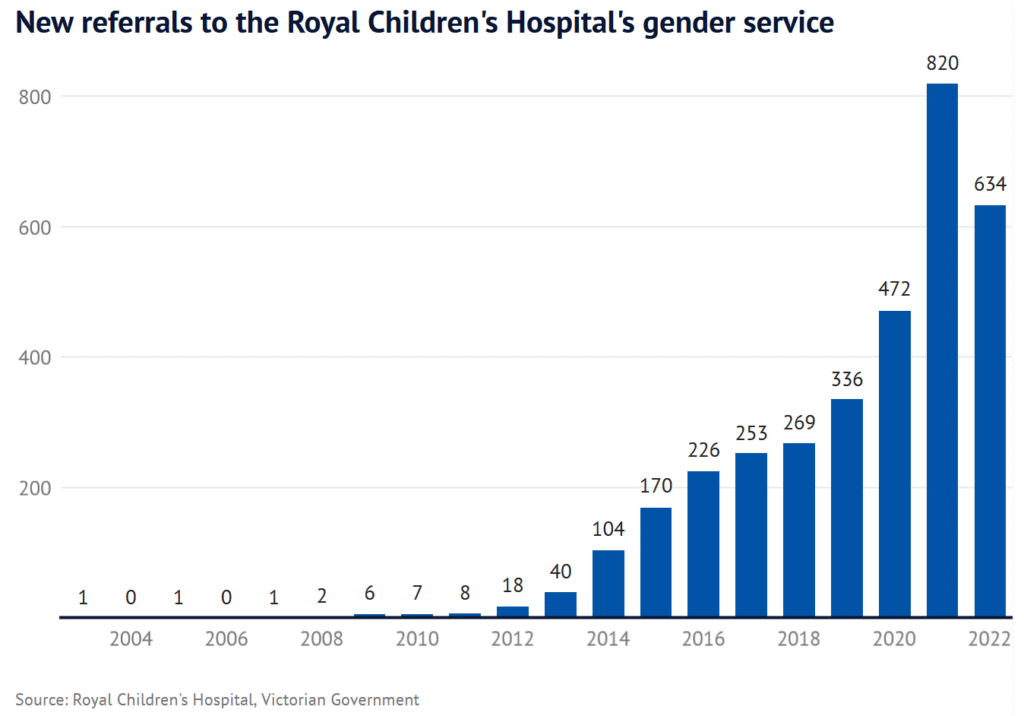
Genspect is concerned that Australia may be facing a delayed but far-reaching wave of regret and detransition, following the steep surge in gender-related distress observed over the past decade. While Australian states and territories do not systematically report data on the number of young people presenting at gender clinics or the medical interventions they undergo, available evidence shows the numbers rising rapidly—as indicated by this graph of data from the Royal Children’s Hospital Melbourne.
Although in previous years, children and adolescents were generally seen at a single gender clinic in each state, this is now changing. More services are opening, and an increasing number of general practitioners (GPs) are initiating and prescribing cross-sex hormones —this shift will make ensuring quality care and optimal outcomes even more challenging.
Need More Information?
Advice for Parents and Detransitioners
Contact Us
If these concerns resonate with you, you want to volunteer, or you need other support, feel free to reach out to Genspect Australia. We also value hearing from Australian clinicians who want to share their experience or join our growing clinical network. You can email us at contact@genspect.org.au.
Join Us
To stay informed about developments in gender medicine in Australia, consider registering with us and subscribing to our substack.
More reading
Our parent and detransitioner support pages have targeted links and recommendations.
- Inspecting Gender, the Genspect Substack has international and Australian news and opinion
- Genspect (international) website provides a wide range of information and resources
- Beyond Trans offers support for parents, families and detransitioners
- The Gender Framework: A Comprehensive Evidence-Based Guide for Professionals and Families (2026). This Genspect-initiated collaboration analyses the origins of gender related distress and an overview of appropriate responses.
Research and Reports
- Society for Evidence-based Gender Medicine (SEGM) analyses research and has prepared a continuing medical education program with videos available
- Stats for Gender maintained by Genspect collates relevant research
- The NHS Cass Report is the most comprehensive review of child gender medicine
- The US HHS Report provides an overview of systematic reviews of evidence which underwent open peer review
- The NHS released 10 new systematic reviews of evidence on hormone use in 2026
Other Australian and International Links
- Gender Question is an Australian website covering transgender medicalisation which has an extensive list of further resources.
- Our Duty parent advocacy organisation operating in Australia and internationally
- Transgender Trend is UK based and advocates for evidence-based approaches
- LS website hosts a summary of links relating to gender identity
- ROGD Boys provides information on boys with gender confusion
- Parents of Desisters documents stories of desistance and provides resources
- Detrans AI provides information and links on detransition as well as an AI tool for analysing discussion on the Reddit detrans page to extract information
- InTRANSigence: Gender Ideology, Social Contagion and the Scandal of Youth Gender Medicine – Dianna Kenny (2025) Explores how psychological and institutional forces shape identity, with an Australian focus.
For Clinicians
- Beyond Transition: A Brief Guidance for Therapists is a Genspect pamphlet that was developed in consultation with experienced clinicians experienced in care of detransitioned individuals.
- Genspect Brief Guidance pamphlets are available for various clinician groups
- Join Therapy First for peer supervision groups, clinical case conferences led by leaders in the field, and discounted webinars and trainings.
- National Association for Practising Psychiatrists (NAPP – Australia) Managing gender dysphoria/incongruence in young people: A guide for health practitioners.
- Society for Evidence-based Gender Medicine (SEGM) analyses research and has prepared a continuing medical education program with videos available
- Stats for Gender maintained by Genspect collates information on relevant research
- Identity and the Foundational Myth: Psychoanalytic Insights into Gender Distress. Marcus Evans (2025)
Genspect Australia is keen to hear from clinicians with experience or interest in managing care for gender questioning youth and/or detransition.
Last updated: June 2026